What Is A Inferior Calcaneal Spur

Overview
A heel spur is a deposit of calcium on the heel bone. This calcification takes the form of a bony protrusion, which can cause considerable pain when standing and walking. This foot problem is closely related to plantar fasciitis, a condition in which the band of fibrous tissue on the bottom of the foot becomes over-stressed. It pulls away from the heel and causes the calcium deposits to form. For this reason, treating a heel spur involves treating the plantar fascia as well.
Causes
Heel spurs are exacerbated by an movements that stretch, twist or impact the plantar ligaments. Running, jumping, standing or walking on hard surfaces with unsupportive shoes, walking barefoot in sand are all activities that can activate heel spurs and plantar fasciitis. Obesity is another factor that increases stress to the plantar ligaments.

Symptoms
If your body has created calcium build-ups in an effort to support your plantar fascia ligament, each time you step down with your foot, the heel spur is being driven into the soft, fatty tissue which lines the bottom of your heel. Heel spur sufferers experience stabbing sensations because the hard protrusion is literally being jabbed into the heel pad. If left untreated, Plantar Fasciitis and heel spurs can erode the fatty pad of the heel and cause permanent damage to the foot. Fortunately, most cases can be resolved without medications or surgeries.
Diagnosis
The diagnosis of heel pain and heel spurs is made by a through history of the course of the condition and by physical exam. Weight bearing x-rays are useful in determining if a heel spur is present and to rule out rare causes of heel pain such as a stress fracture of the heel bone, the presence of bone tumors or evidence of soft tissue damage caused by certain connective tissue disorders.
Non Surgical Treatment
A conventional treatment for a heel spur is a steroid injection. This treatment, however, isn?t always effective because of the many structures in the heel, making it a difficult place for an injection. If this treatment goes wrong, it can make the original symptoms even worse. Another interesting means of treatment is Cryoultrasound, an innovative electromedical device that utilizes the combination of two therapeutic techniques: cryotherapy and ultrasound therapy. Treatments with Cryoultrasound accelerate the healing process by interrupting the cycle and pain and spasms. This form of therapy increases blood circulation and cell metabolism; it stimulates toxin elimination and is supposed to speed up recovery.
Surgical Treatment
In a small number of cases (usually less than 5 percent), patients may not experience relief after trying the recommendations listed above. It is important that conservative treatments (such as those listed above) be performed for AT LEAST a year before considering surgery. Time is important in curing the pain from heel spurs, and insufficient treatment before surgery may subject you to potential complications from the procedure. If these treatments fail, your doctor may consider an operation to loosen the plantar fascia, called a plantar fascia release.
Prevention
Prevention of heel spur syndrome may be best by finding a good supportive shoe. Never go barefoot or wear a flat soled shoe. There are many over the counter arch supports that give increased support for your feet. Usually when there is excessive pronation the Achilles Tendon contracts or becomes shortened over time since it is not being used fully. The shortened Achilles Tendon is called an equinus deformity. By keeping this tendon stretched it may decrease some of the tension in the foot. Some theories believe the Achilles Tendon and plantar fascia is continuous. Before you get up from rest, stretch out your Achilles and the plantar fascia. You may attempt to spell the alphabet with your foot and ankle, use a towel against pressure on your foot, or roll a can of soup or sodapop on the ground. Ice may work well at the times of severe pain. For a chronic pain, or longer lasting pain heat therapy may improve the condition.
Hammer Toe Pain When Ever Running
 Overview
Overview
A Hammer toes is a deformity of the second, third or hammertoe fourth toes in which the main toe joint is bent upward like a claw. Initially, hammertoes are flexible and can be corrected with simple measures. Left untreated, they can become fixed and require surgery. Hammertoe results from shoes that don?t fit properly or a muscle imbalance, usually in combination with one or more other factors. Muscles work in pairs to straighten and bend the toes. If the toe is bent and held in one position long enough, the muscles tighten and can?t stretch out.
Causes
Your shoes, your genetic predisposition, an underlying medical condition or all of these can make you susceptible to developing one of these deformities of the toes. The genes your parents gave you. When it comes to genetics, the foot type you?re born with predisposes you to developing this type of joint deformity over a lifetime. For many, a flat flexible foot leads to hammertoes as the foot tries to stabilize against a flattening arch. Those with high arches can also form hammertoes as the extensor tendons overpower the flexors.
 Symptoms
Symptoms
Some people never have troubles with hammer toes. In fact, some people don't even know they have them. They can become uncomfortable, especially while wearing shoes. Many people who develop symptoms with hammer toes will develop corns, blisters and pain on the top of the toe, where it rubs against the shoe or between the toes, where it rubs against the adjacent toe. You can also develop calluses on the balls of the feet, as well as cramping, aching and an overall fatigue in the foot and leg.
Diagnosis
Hammertoes are progressive, they don?t go away by themselves and usually they will get worse over time. However, not all cases are alike, some hammertoes progress more rapidly than others. Once your foot and ankle surgeon has evaluated your hammertoes, a treatment plan can be developed that is suited to your needs.
Non Surgical Treatment
Non-surgical methods for hammer toes (claw toes) are aimed at decreasing symptoms (i.e., pain and/or calluses) and/or limiting the progression into a larger problem. Simple treatments patients can do are wear supportive shoes. Use an arch support. Wear shoes with a wide toe box. Modify activities. Spot stretch shoes. Periodic callus care.
Surgical Treatment
Curative treatment of hammertoes varies depending upon the severity of the deformity. When the hammertoe is flexible, a simple tendon release in the toe works well. The recovery is rapid often requiring nothing more that a single stitch and a Band-Aid. Of course if several toes are done at the same time, the recovery make take a bit longer.
 Prevention
Prevention
These tips may help you buy the right shoes. Buy shoes at the end of the day. Your feet are smaller in the morning and swell throughout the day. Don't assume your shoe size hasn't changed. As you age, your shoe size may change, especially the width. Measure both feet and buy for the larger foot. Ask for just the right fit. A shoe repair store can stretch shoes in tight spots.
Hammer Toe Pain When Ever Running
 Overview
Overview
A hammertoe is a deformity in the foot, causing the second, third, or fourth toe to be permanently bent in the middle joint, causing the toe to resemble a hammer (hence, its name!) or a claw. They are most commonly found in women who wear narrow shoes, such as high heels, that cause the toes to bend unnaturally for extended periods of time. A hammertoes may be difficult or painful to move, and the skin may become callused from rubbing against the inside of the shoe. In fact, there are two types of hammertoe: flexible and rigid. Flexible hammertoes can still move at the joint and are indicative of an earlier, milder form of the problem. Rigid hammertoes occur when the tendon no longer moves, and at this stage, surgery is usually necessary to fix the problem.
Causes
Your toe contains two joints that allow it to bend at the middle and bottom. A hammertoe occurs when the middle joint becomes dislocated. Common causes of this joint dislocation include a toe injury, arthritis, a high foot arch, wearing shoes that don?t fit properly, tightened ligaments or tendons in the foot, pressure from a bunion (when your big toe points inward toward your second toe) Spinal cord or peripheral nerve damage may cause all of your toes to curl downward.
 Symptoms
Symptoms
Well-developed hammertoes are distinctive due to the abnormal bent shape of the toe. However, there are many other common symptoms. Some symptoms may be present before the toe becomes overly bent or fixed in the contracted position. Often, before the toe becomes permanently contracted, there will be pain or irritation over the top of the toe, particularly over the joint. The symptoms are pronounced while wearing shoes due to the top of the toe rubbing against the upper portion of the shoe. Often, there is a significant amount of friction between the toe and the shoe or between the toe and the toes on either side of it. The corns may be soft or hard, depending on their location and age. The affected toe may also appear red with irritated skin. In more severe cases, blisters or open sores may form. Those with diabetes should take extra care if they develop any of these symptoms, as they could lead to further complications.
Diagnosis
The earlier a hammertoe is diagnosed, the better the prognosis and treatment options. Your doctor will be able to diagnose your hammertoe with a simple examination of the foot and your footwear. He or she may take an x-ray to check the severity of the condition. You may also be asked about your symptoms, your normal daily activities, and your medical and family history.
Non Surgical Treatment
You can usually use over-the-counter cushions, pads, or medications to treat bunions and corns. However, if they are painful or if they have caused your toes to become deformed, your doctor may opt to surgically remove them. If you have blisters on your toes, do not pop them. Popping blisters can cause pain and infection. Use over-the-counter creams and cushions to relieve pain and keep blisters from rubbing against the inside of your shoes. Gently stretching your toes can also help relieve pain and reposition the affected toe.
Surgical Treatment
Surgery involves removing a small section of bone from the affected joint through a procedure called arthroplasty. Arthrodesis hammertoe may also be performed to treat hammertoes, which involves fusing together one of the joints in the toe in order to keep it straight. This procedure requires the use of a metal pin to hold the toe in position while it heals.
Know About Over-Pronation Of The Foot
Overview
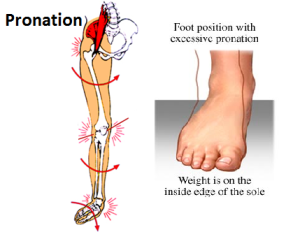
Simply put, over-pronation is an excessive or poorly timed pronation which is part of the regular stride. Pronation is when the foot rolls inwards and the arch compresses as part of your normal walking motion. Pronation is necessary for shock absorption to transmit forces up and down our legs. When someone over-pronates, the foot rolls inwards to a greater degree and the arch flattens: this causes the knee and hip to come out of alignment and reduces the function of all the bones in the feet.

Causes
Generally fallen arches are a condition inherited from one or both parents. In addition, age, obesity, and pregnancy cause our arches to collapse. Being in a job that requires long hours of standing and/or walking (e.g. teaching, retail, hospitality, building etc) contributes to this condition, especially when standing on hard surfaces like concrete floors. Last, but not least unsupportive footwear makes our feet roll in more than they should.
Symptoms
Symptoms can manifest in many different ways. The associated conditions depend on the individual lifestyle of each patient. Here is a list of some of the conditions associated with over Pronation. Hallux Abducto Valgus (bunions). Hallux Rigidus (stiff 1st toe). Arch Pain. Heel Pain (plantar Facsitus). Metatarsalgia (ball of the foot pain). Ankle Sprains. Shin Splints. Achilles Tendonitis. Osteochondrosis. Knee Pain. Corns & Calluses. Flat Feet. Hammer Toes.
Diagnosis
So, how can you tell if you have overpronation, or abnormal motion in your feet, and what plantar fasciitis treatment will work to correct it? Look at your feet. While standing, do you clearly see the arch on the inside of your foot? If not, and if the innermost part of your sole touches the floor, then your feet are overpronated. Look at your (running/walking) shoes. If your shoes are more worn on the inside of the sole in particular, then pronation may be a problem for you. Use the wet foot test. Wet your feet and walk along a section of pavement, then look at the footprints you leave behind. A normal foot will leave a print of the heel connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot.
Non Surgical Treatment
Treatment with orthotics will provide the required arch support to effectively reduce excessive pronation and restore the foot and its posture to the right biomechanical position. It should be ensured that footwear has sufficient support, for example, shoes should have a firm heel counter to provide adequate control.
Prevention
Custom-made orthotics supports not only the arch as a whole, but also each individual bone and joint that forms the arch. It is not enough to use an over-the-counter arch support, as these generic devices will not provide the proper support to each specific structure of the arch and foot. Each pronated foot?s arch collapses differently and to different degrees. The only way to provide the support that you may need is with a custom-made device. This action of the custom-made orthotic will help to prevent heel spurs, plantar fasciitis, calluses, arch pain, and weakness of the entire foot.
The Cause For Adult Aquired FlatFeet
Overview
Have you noticed that the medial arch of your foot is becoming flatter when you walk? You may be developing adult acquired flat foot. This condition is typically caused by a problem with a tendon on the medial side of your foot called the Posterior Tibial Tendon that is not functioning well. You may experience pain in the inner side of your foot when you walk. The affected foot appears to roll outwards (the sole of the foot is trying to face outwards) when you walk. This is called over-pronation of the foot. The back of your heel may start to point outwards (heel valgus). Over time you may lose the ability to tip toe on that foot as the posterior tibial tendon stretches out and it may eventually tear.

Causes
Flat feet causes greater pressure on the posterior tibial tendon than normal. As the person with flat feet ages, the muscles, tendons and ligaments weaken. Blood supplies diminish as arteries narrow. These conditions are magnified for obese patients because of their increased weight and atherosclerosis. Finally, the tendon gives out or tears. Most of the time, this is a slow process. Once the posterior tibial tendon and ligaments stretch, body weight causes the bones of the arch to move out of position. The foot rotates inward (pronation), the heel bone is tilted to the inside, and the arch appears collapsed. In some cases, the deformity progresses until the foot dislocates outward from the ankle joint.
Symptoms
The first stage represents inflammation and symptoms originating from an irritated posterior tibial tendon, which is still functional. Stage two is characterized by a change in the alignment of the foot noted on observation while standing (see above photos). The deformity is supple meaning the foot is freely movable and a ?normal? position can be restored by the examiner. Stage two is also associated with the inability to perform a single-leg heel rise. The third stage is dysfunction of the posterior tibial tendon is a flatfoot deformity that becomes stiff because of arthritis. Prolonged deformity causes irritation to the involved joints resulting in arthritis. The fourth phase is a flatfoot deformity either supple (stage two) or stiff (stage 3) with involvement of the ankle joint. This occurs when the deltoid ligament, the major supporting structure on the inside of the ankle, fails to provide support. The ankle becomes unstable and will demonstrate a tilted appearance on X-ray. Failure of the deltoid ligament results from an inward displacement of the weight bearing forces. When prolonged, this change can lead to ankle arthritis. The vast majority of patients with acquired adult flatfoot deformity are stage 2 by the time they seek treatment from a physician.
Diagnosis
The adult acquired flatfoot, secondary to posterior tibial tendon dysfunction, is diagnosed in a number of ways with no single test proven to be totally reliable. The most accurate diagnosis is made by a skilled clinician utilizing observation and hands on evaluation of the foot and ankle. Observation of the foot in a walking examination is most reliable. The affected foot appears more pronated and deformed compared to the unaffected foot. Muscle testing will show a strength deficit. An easy test to perform in the office is the single foot raise. A patient is asked to step with full body weight on the symptomatic foot, keeping the unaffected foot off the ground. The patient is then instructed to "raise up on the tip toes" of the affected foot. If the posterior tibial tendon has been attenuated or ruptured, the patient will be unable to lift the heel off the floor and rise onto the toes. In less severe cases, the patient will be able to rise on the toes, but the heel will not be noted to invert as it normally does when we rise onto the toes. X-rays can be helpful but are not diagnostic of the adult acquired flatfoot. Both feet - the symptomatic and asymptomatic - will demonstrate a flatfoot deformity on x-ray. Careful observation may show a greater severity of deformity on the affected side.
Non surgical Treatment
Flatfoot can be treated with a variety of methods, including modified shoes, orthotic devices, a brace or cast, anti-inflammatory medications or limited steroid injections, rest, ice, and physical therapy. In severe cases, surgery may be necessary.

Surgical Treatment
Although non-surgical treatments can successfully manage the symptoms, they do not correct the underlying problem. It can require a life-long commitment to wearing the brace during periods of increased pain or activity demands. This will lead a majority of patients to choose surgical correction of the deformity, through Reconstructive Surgery. All of the considerations that were extremely important during the evaluation stage become even more important when creating a surgical plan. Generally, a combination of procedures are utilized in the same setting, to allow full correction of the deformity. Many times, this can be performed as a same-day surgery, without need for an overnight hospital stay. However, one or two day hospital admissions can be utilized to help manage the post-operative pain. Although the recovery process can require a significant investment of time, the subsequent decades of improved function and activity level, as well as decreased pain, leads to a substantial return on your investment.
Just What Can Cause Tendinitis In The Achilles ?
Overview
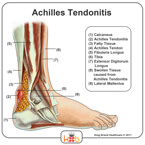 The Achilles tendon is the largest tendon in the body. It connects the calf muscles to the heel and is active during almost all activities including walking, jumping, and swimming. This dense tendon can withstand large forces, but can become inflamed and painful during periods of overuse. Pain results from inflammation (tendonitis) or a degenerating tendon (tendinosis). Achilles tendon pathologies include rupture and tendonitis. Many experts now believe, however, that tendonitis is a misleading term that should no longer be used, because signs of true inflammation are almost never present on histologic examination. Instead, the following histopathologically determined nomenclature has evolved. Paratenonitis: Characterized by paratenon inflammation and thickening, as well as fibrin adhesions. Tendinosis: Characterized by intrasubstance disarray and degeneration of the tendon.
The Achilles tendon is the largest tendon in the body. It connects the calf muscles to the heel and is active during almost all activities including walking, jumping, and swimming. This dense tendon can withstand large forces, but can become inflamed and painful during periods of overuse. Pain results from inflammation (tendonitis) or a degenerating tendon (tendinosis). Achilles tendon pathologies include rupture and tendonitis. Many experts now believe, however, that tendonitis is a misleading term that should no longer be used, because signs of true inflammation are almost never present on histologic examination. Instead, the following histopathologically determined nomenclature has evolved. Paratenonitis: Characterized by paratenon inflammation and thickening, as well as fibrin adhesions. Tendinosis: Characterized by intrasubstance disarray and degeneration of the tendon.
Causes
Like any muscle or tendon in the body, the older we get, the more likely we are to sustain an injury. So middle-aged men and women are most at risk, with a slightly higher risk factor attributed to males. Those who participate in more intense athletic activities like high impact sports (tennis, running, basketball) are most susceptible to the injury. Certain underlying medical conditions can also be a contributing factor. Diabetics are more at risk of suffering from Achilles Tendinitis, as are those who are not in great physical shape. Some antibiotics, particularly fluoroquinolones can make one more likely to suffer a strained Achilles Tendon.
Symptoms
Achilles tendinitis symptoms present as mild to severe pain or swelling near the ankle. The pain may lead to weakness and decreased mobility, symptoms that increase gradually while walking or running. Over time, the pain worsens, and stiffness in the tendon may be noted in the morning. Mild activity may provide relief. Physical exam may reveal an audible cracking sound when the Achilles tendon is palpated. The lower leg may exhibit weakness. A ruptured or torn Achilles tendon is severely painful and warrants immediate medical attention. The signs of a ruptured or torn Achilles tendon include. Acute, excruciating pain. Impaired mobility, unable to point the foot downward or walk on the toes. Weight bearing or walking on the affected side is not possible.
Diagnosis
A doctor or professional therapist will confirm a diagnosis, identify and correct possible causes, apply treatment and prescribe eccentric rehabilitation exercises. An MRI or Ultrasound scan can determine the extent of the injury and indicate a precise diagnosis. Gait analysis along with a physical assessment will identify any possible biomechanical factors such as over pronation which may have contributed to the achilles tendonitis and training methods will be considered. Biomechanical problems can be corrected with the use of orthotic inserts and selection of correct footwear.
Nonsurgical Treatment
Treatment of Achilles tendonitis begins with resting the tendon to allow the inflammation to settle down. In more serious situations, adequate rest may require crutches or immobilization of the ankle. Learn more about different treatments for Achilles tendonitis, including ice, medications, injections, and surgery.
Surgical Treatment
Percutaneous Achilles Tendon Surgery. During this procedure the surgeon will make 3 to 4 incisions (approx. 2.5 cm long) on both sides of the Achilles tendon. Small forceps are used to free the tendon sheath (the soft tissue casing around your Achilles tendon) to make room for the surgeon to stitch/suture any tears. Skilled surgeons may perform a percutaneous achilles tendon surgery with ultrasound imaging techniques to allow for blink suturing with stab incisions made by a surgical suture needle. This procedure can be done in 3 different ways depending on the preference and experience of your surgeon. Instead of making several 2.5 cm incisions for this procedure, some surgeons will use guided imaging with an ultrasound to see the Achilles tendon tissue without having to open up your ankle. For this technique, they will use a surgical needle to repeatedly stab your Achilles tendon. These "stab incisions" will allow the surgeon to "blindly" suture your tendon without seeing the actual tissue. As another option - some surgeons will only make 1 to 3 incisions for smaller surgical implements to repair your tendon while relying on imaging ultrasound to see your damaged tissue. During either procedure the use of ultrasound imaging or endoscopic techniques requires a very skilled surgeon.
Prevention
Stretching of the gastrocnemius (keep knee straight) and soleus (keep knee bent) muscles. Hold each stretch for 30 seconds, relax slowly. Repeat stretches 2 - 3 times per day. Remember to stretch well before running strengthening of foot and calf muscles (eg, heel raises) correct shoes, specifically motion-control shoes and orthotics to correct overpronation. Gradual progression of training programme. Avoid excessive hill training. Incorporate rest into training programme.
An Achilles Tendon Rupture How Would I Know I Have Got One?
Overview

The Achilles tendon is the largest tendon in the body. It connects your calf muscles to your heel bone and is used when you walk, run, and jump. Although the Achilles tendon can withstand great stresses from running and jumping, it is vulnerable to injury. A rupture of the tendon is a tearing and separation of the tendon fibers so that the tendon can no longer perform its normal function.
Causes
Ruptured Achilles tendons may result from falling from a height or down a hole. Increasing training intensity abruptly, boosting distance, frequency or duration by more than 10% a week. Failing to stretch before and after exercise. Repetitive training, especially uphill running. Deyhydration, which causes cramping and tightness in the calves. Taking antibiotics. Improper footwear. Explosive movements in competitive sports like basketball, soccer or track & field.
Symptoms
Symptoms usually come on gradually. Depending on the severity of the injury, they can include Achilles pain, which increases with specific activity, with local tenderness to touch. A sensation that the tendon is grating or cracking when moved. Swelling, heat or redness around the area. The affected tendon area may appear thicker in comparison to the unaffected side. There may be weakness when trying to push up on to the toes. The tendon can feel very stiff first thing in the morning (care should be taken when getting out of bed and when making the first few steps around the house). A distinct gap in the line of the tendon (partial tear).
Diagnosis
Most Achilles tendon ruptures occur in people between 30 and 50 years old and such injuries are often sport-related. If you suspect an Achilles injury, it is best to apply ice, elevate the leg, and see a specialist. One of the first things the doctor will do is evaluate your leg and ankle for swelling and discoloration. You may feel tenderness and the doctor may detect a gap where the ends of the tendon are separated. In addition to X-rays, the calf squeeze, or Thompson test, will be performed to confirm an Achilles tendon rupture. With your knee bent, the doctor will squeeze the muscles of your calf and if your tendon is intact the foot and ankle will automatically flex downward. In the case of a ruptured Achilles there will be no movement in the foot and ankle during the test.
Non Surgical Treatment
Once a diagnosis of Achilles tendon rupture has been confirmed, a referral to an orthopaedic specialist for treatment will be recommended. Treatment for an Achilles tendon rupture aims to facilitate the torn ends of the tendon healing back together again. Treatment may be non-surgical (conservative) or surgical. Factors such as the site and extent of the rupture, the time since the rupture occurred and the preferences of the specialist and patient will be considered when deciding which treatment will be undertaken. Some cases of rupture that have not responded well to non-surgical treatment may require surgery at a later stage. The doctor will immobilise the ankle in a cast or a special hinged splint (known as a ?moon boot?) with the foot in a toes-pointed position. The cast or splint will stay in place for 6 - 8 weeks. The cast will be checked and may be changed during this time.

Surgical Treatment
Surgery offers important potential benefits. Besides decreasing the likelihood of re-rupturing the Achilles tendon, surgery often increases the patient?s push-off strength and improves muscle function and movement of the ankle. Various surgical techniques are available to repair the rupture. The surgeon will select the procedure best suited to the patient. Following surgery, the foot and ankle are initially immobilized in a cast or walking boot. The surgeon will determine when the patient can begin weightbearing. Complications such as incision-healing difficulties, re-rupture of the tendon, or nerve pain can arise after surgery. Whether an Achilles tendon rupture is treated surgically or non-surgically, physical therapy is an important component of the healing process. Physical therapy involves exercises that strengthen the muscles and improve the range of motion of the foot and ankle.
Causes Indicators And Therapy For Achilles Tendon Ruptures
Overview

The Achilles tendon is the largest and strongest tendon in the human body. The Achilles tendon connects the heel bone (calcaneus) to the muscles at the back of the calf (using gastrocnemius and soleus muscles). The synchronous function of the tendon and calf muscles is critical for activities like jumping, running, standing on the toe, and climbing stairs. When climbing stairs or running, the forces within the tendon have been measured and indicate that the structure is able to withstand at least 10 times the body weight of the individual. The function of the Achilles tendon is to help raise your heel as you walk. The tendon also assists in pushing up the toes and lifting the rear of the heel. Without an intact Achilles tendon, almost any motion with the ankle (for example, walking or running) is difficult.
Causes
Your Achilles tendon helps you point your foot downward, rise on your toes and push off your foot as you walk. You rely on it virtually every time you move your foot. Rupture usually occurs in the section of the tendon located within 2 1/2 inches (about 6 centimeters) of the point where it attaches to the heel bone. This section may be predisposed to rupture because it gets less blood flow, which also may impair its ability to heal. Ruptures often are caused by a sudden increase in the amount of stress on your Achilles tendon. Common examples include increasing the intensity of sports participation, especially in sports that involve jumping, falling from a height, stepping into a hole.
Symptoms
Symptoms of an Achilles tendon injury are as follows. Pain along the back of your foot and above your heel, especially when stretching your ankle or standing on your toes; with tendinitis, pain may be mild and worsen gradually. If you rupture the tendon, pain can be abrupt and severe. Tenderness. Swelling. Stiffness. Hearing a snapping or popping noise during the injury. Difficulty flexing your foot or pointing your toes (in complete tears of the tendon).
Diagnosis
The doctor may look at your walking and observe whether you can stand on tiptoe. She/he may test the tendon using a method called Thompson?s test (also known as the calf squeeze test). In this test, you will be asked to lie face down on the examination bench and to bend your knee. The doctor will gently squeeze the calf muscles at the back of your leg, and observe how the ankle moves. If the Achilles tendon is OK, the calf squeeze will make the foot point briefly away from the leg (a movement called plantar flexion). This is quite an accurate test for Achilles tendon rupture. If the diagnosis is uncertain, an ultrasound or MRI scan may help. An Achilles tendon rupture is sometimes difficult to diagnose and can be missed on first assessment. It is important for both doctors and patients to be aware of this and to look carefully for an Achilles tendon rupture if it is suspected.
Non Surgical Treatment
Medical therapy for a patient with an Achilles tendon rupture consists of rest, pain control, serial casting, and rehabilitation to maximize function. Ongoing debate surrounds the issue of whether medical or surgical therapy is more appropriate for this injury. Conservative management of Achilles tendinosis and paratenonitis includes the following. Physical therapy. Eccentric exercises are the cornerstone of strengthening treatment, with most patients achieving 60-90% pain relief. Orthotic therapy in Achilles tendinosis consists of the use of heel lifts. Nonsteroidal anti-inflammatory drugs (NSAIDs). Tendinosis tends to be less responsive than paratenonitis to NSAIDs. Steroid injections. Although these provide short-term relief of painful symptoms, there is concern that they can weaken the tendon, leading to rupture. Vessel sclerosis. Platelet-rich plasma injections. Nitric oxide. Shock-wave therapy.

Surgical Treatment
In general, for complete tear of the tendon, surgery is recommended. For partial tears, nonsurgical treatment is recommended. However, the selection of treatment depends on the patient, age, level of activity, and other risk factors. Surgery for Achilles tendon rupture is now routine and well established. Surgery is generally suggested for the young, healthy and active individuals. For athletes, surgery is often the first choice of treatment. The Achilles tendon can be repaired surgically by either a closed or open technique. With the open technique, an incision is made to allow for better visualization and approximation of the tendon. With the closed technique, the surgeon makes several small skin incisions through which the tendon is repaired. Irrespective of type of treatment, a short leg cast (plaster) is applied on the operated ankle after completion of the procedure. The advantages of a surgical approach includes a decreased risk of re-rupture rate (0%-5%) the majority of individuals can return to their original sporting activities (within a short time), and most regain their strength and endurance. Disadvantages of a surgical approach include hospital admission, wound complications (for example, skin sloughing, infection, sinus tract formation, sural nerve injury), higher costs, and hospital admission.
Prevention
To help reduce your chance of getting Achilles tendon rupture, take the following steps. Do warm-up exercises before an activity and cool down exercises after an activity. Wear proper footwear. Maintain a healthy weight. Rest if you feel pain during an activity. Change your routine. Switch between high-impact activities and low-impact activities. Strengthen your calf muscle with exercises.
Make a Free Website with Yola.